
Editor’s Note: This text is a transcript of the course, ALS: Medications and Oral Care, presented by Denise Dougherty, MA, SLP.
Learning Outcomes
After this course, participants will be able to:
- Describe rationale and list side effects of medications/complementary alternative medicine for ALS
- Identify strategies to manage secretions
- Explain how to educate patients and families about the importance of mouth care.
Overview
This is Part 1 of a three-part series on amyotrophic lateral sclerosis (ALS), and we will be talking about the medications and oral care. My email address is listed in the handout. If you have any questions or comments following the seminar please feel free to email me.
As for disclosures, I am receiving an honorarium for the presentation. I make my living in private practice, and also as a forensic speech pathologist. My non-financial disclosure is that I work with Quality Insights of Pennsylvania, on medication review and communication with the Centers for Medicare and Medicaid Services (CMS).
We have three parts to this series. Part 1 will cover medications and oral care. Part 2 will discuss the pros and cons of exercise and the role of therapeutic exercise with this type of individual. There have been some interesting studies on that in the last several years. In Part Three, we will look at the impact on nutrition, and the different strategies that can be used with clients to maintain nutrition and hydration. Part 3 will also discuss the pros and cons of the percutaneous endoscopic gastrostomy (PEG) tube placement, which is very important in this population.
After completing this course, you should be able to describe the rationale and list the side effects of medications and what we call complementary alternative medication (CAM) for ALS. You should be able to identify strategies to manage secretions and explain how you would educate patients and families about the importance of mouth care. In regards to mouth care, it does not matter what disorder or disease process we are dealing with; mouth care is critical for all of our patients with dysphagia.
ALS - Introduction
ALS is one of the progressive, debilitating neurodegenerative diseases, so it’s important to know what is available as far as medications and complementary alternative medications. Many times, patients with ALS, or any of the motor neuron diseases, will supplement their traditional medications with herbs or supplements. It is very important to know what they are consuming because there are side effects, not just of the complementary alternative medication, but from mixing it with traditional prescriptions. Patients may not recognize how dangerous this interaction can be. We also need to know about saliva management strategies, and the importance of mouth care for our patients.
In 1874, French physician Jean Charcot was the first one to link the symptoms of ALS to groups of nerves that were affected. It just so happened that his housekeeper was diagnosed with ALS, so he was able to observe the clinical manifestations of that disease process as she went through the various stages. His observations and descriptions are still very accurate today.
Neurons
In ALS, we definitely need to look at neurons. The neurons facilitate neurotransmission between the upper and the motor neurons, sending messages down from the brain and the brainstem to the muscles in the body. Now, many of these neurons are very large, with long axons. These neurons have high metabolic needs; that is, they have high energy demands. Plus, the longer the axon, the more vulnerable that neuron is to toxins because there is a larger surface area. Any exposure to environmental toxins, therefore, can take its toll.
Figure 1 shows the communication circle that we see.
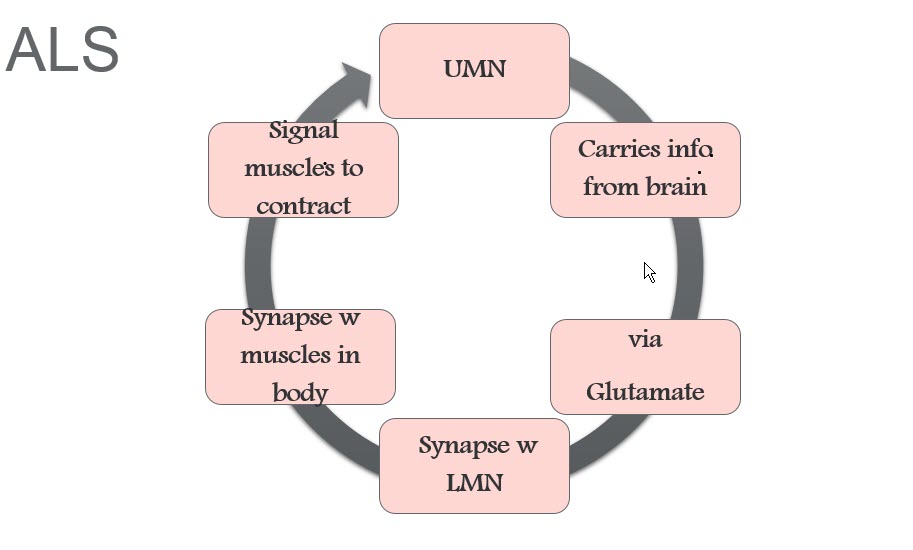
Figure 1. ALS communication circle.
The upper motor neurons (UMN) in the brain and the brainstem send information to the lower motor neurons (LMN). Glutamate is used to transmit that information. That is really important when we are talking about ALS patients because often they have much more glutamate than is normal. That is why they take a certain medication meant to slow down production of glutamate. But it is a very important neurotransmitter when it is produced in the correct amounts. Information is transmitted through those synapses between LMN and the muscles in the body, and the muscles are told to contract.
Why ALS?
There are many different theories about why people develop ALS. Many times the same theories are proposed for all of the motor neuron disorders or diseases. Some of these in Figure 2 - oxidative stress, toxins and genetics - you will recognize, but there are some that were surprising to me. These include sports trauma, excessive exercise, and excitotoxicity.
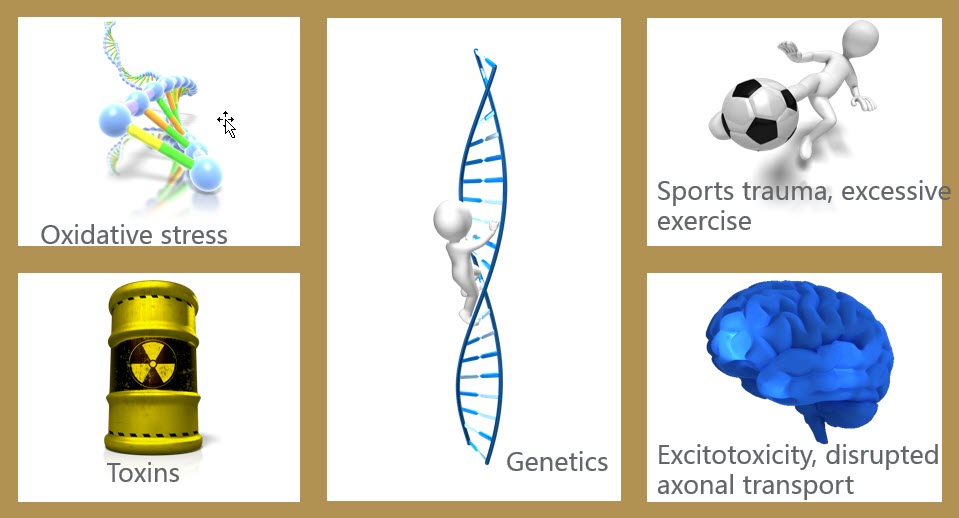
Figure 2. ALS theories.
Excitotoxicity and Disrupted Axonal Transport
Let's look at excitotoxicity and disrupted axonal transport. If you have too much glutamate, the neurons get too excited and overreact. That contributes to neuronal death because they basically exhaust themselves. With disrupted axonal transport, things slow down such that there is a backup of proteins and lipids right at the synapses. There is so much buildup that it creates toxicity at the level of the synapses, and disrupts the whole function. Those are some of the theories.
Toxins
Toxins are typically thought of in terms of pesticides, heavy metals, household chemicals, or mercury. If you grew up in the 1950s and 1960s like I did and you went to the dentist, you ended up with a mouth full of those silver (amalgam) fillings. Those have been shown to possibly predispose you to ALS. There are a number of dental practices that advertise that they are able to remove those fillings and replace them with what is the standard today. They even have rooms set up specifically to control the dust.
Sports Trauma and Excessive Exercise
Let's take a look at sports trauma and excessive exercise. Studies have found that there is a high incidence of ALS in athletes. One study showed that Italian soccer players have a six times greater risk for ALS. There was also an Irish cohort. Note that those are countries where soccer is very popular. They have looked at the damage and the trauma to the muscles and the tendons of the legs due to the sports activity, as well as the different exercises they use to stay functioning as an athlete. They have also hypothesized that when you have scrapes and cuts, ticks can enter the body. In addition, whenever you are playing and you fall on the field, your face is now in contact with whatever the field has been treated with so you can inhale those toxic chemicals. They have studied the amount of exercise that football players do. There is also some concern about medications, such as performance-enhancing drugs; a prescription med that is perfectly legal but is taken for too long or in larger doses than are appropriate; or, potentially, medication for any kind of trauma that has been experienced. So there are several concerns related to sports trauma and exercise.
Oxidative Stress
There is a reason why people should take antioxidants and try to incorporate foods high in antioxidants into the diet. Oxidative stress has been studied in a variety of motor neuron diseases. Approximately 2% of oxygen metabolized (consumed) produces something called reactive oxygen species (ROS). That is normal. Your body does not produce more than it can handle. But if something happens that throws the system out of balance, you could end up with too much ROS, and the body will not know what to do with it. You then end up having oxidation of lipids and proteins. The cells are damaged by that oxidation, causing damage to the DNA and RNA. It requires a lot of metabolic energy to repair that damage, and if it is not repaired sufficiently, those cells become dysfunctional. That means two things happen. First, your body activates calcium channels, such that you are producing more calcium than you should. Second, the calcium pumps have been deactivated so you cannot get rid of the calcium. You end up with an overabundance - an abnormally high intracellular level of calcium - and that causes cellular death.
There are many different theories, and many times the same theories pop up for Parkinson's and Huntington's disease that is related to ALS. Possibly, we are looking at the same type of damage for these different diseases.
Supplements and Medications
As mentioned earlier, patients may be experimenting with herbs and supplements. Sometimes, we don’t know that and are at a loss when we see something happen to their level of functioning or their health, and we cannot explain why. It could be that they are consuming supplements or herbs that are creating a bad interaction with their traditional medications. Even when working in a facility where the medications that patients take can be controlled to a large degree, it is still very possible for families to sneak something in that we are not aware of. There have been several facilities in my area where families were bringing things in and the staff was not aware of it. Things like that happen. But in a facility, for the most part, you tend to know what they are taking and whether there has been an increase or decrease in the dosage.
It is with home health patients and outpatients that you need to be a bit more insistent: “Tell me what you are consuming.” Many times, they don’t really like to tell us about the herbs and supplements because they know some people tend to frown on that as an approach. I always tell them that there is no judgment and they are free to treat their own disorder or disease process in any way they choose. But because there could be a side effect or interaction with medications they are currently taking, it is helpful for me to know about them. Some side effects create swelling of the face and the lips and the tongue, which is not a good thing for our patients who have swallowing problems, or even the healthy patient. So we need to know.
Apps
There are applications available, including one called the Natural Medicines Comprehensive Database, that provide information on the efficacy and safety of supplements and possible drug-supplement interactions. For example, if the patient is consuming St. John's wort, what does that do? The app also indicates if the supplement has been verified by the United States Pharmacopeial Convention (USP). They review the listed ingredients and verify that those are exactly what are in that capsule or tablet.
Creatine
The two supplements that I have seen studied in the literature are creatine and Vitamin E. Both of these have particular side effects even when taken alone, as well as when you combine them with other medications.
Creatine is naturally produced in your kidneys, liver, and pancreas. We need to recognize that as we age, those body parts do not function like they did when we were younger. They shrink in size, and their blood supply also changes. If you are taking creatine, you have to drink plenty of fluids because one of the side effects is dehydration. Studies looking at the impact of creatine have not really seen results that indicate it improves your survival or improves your level of functioning. Nothing in the literature has substantiated the use of this. But if patients read on a blog that somebody got better, then they are going to give it a try. In addition to dehydration, the side effects of creatine can include muscle cramps, electrolyte imbalance, and swelling of the lips, tongue, and face.
Vitamin E
With vitamin E, there have been several studies conducted looking at consuming it in combination with medications that your patients might be taking. Many ALS patients take a drug called Riluzole. Studies have looked at taking vitamin E along with Riluzole and compared it to taking Riluzole by itself. These studies did not find any difference in survival or functional outcomes achieved by giving vitamin E. But again, our patients may just go ahead and do it anyway.
Too much vitamin E can cause dangerous side effects. It causes fatigue, weakness, blurred vision, and diarrhea. For individuals with ALS, there is already a fatigue factor and a weakness factor. Taking vitamin E may, therefore, complicate their ability to consume food and liquids safely at mealtimes. When there is a diarrhea component, many of our patients will refuse to eat because they know if they do, they are going to be spending some time in the bathroom, and that is not what they want. Not eating, of course, is not good for them.
Resources
There are some places you can look for information on medications. One example is a book called Drugs and Dysphagia that is available in some of the speech catalogs. It is very small and is a great desk reference. It has chapters on classes of drugs and gives foundational information.
If you have electronic medical record (EMR) systems, many of them have their own drug interaction checker. But in some facilities, they can turn that off. I know in our home health facility, we have the electronic medical records and we have access to the drug interaction checker. It may not be activated in the system that you are using.
WebMD, RXList, Medscape.com, and Drugs.com are some other sights with medication information. Those last two specifically not only have an interaction checker for between-prescription drug interactions; they also allow you to check interactions with some herbs and over-the-counter medications. You can type in every medication your patient is consuming and then print out a list of “bad things that happen when you combine these particular medications and/or supplements.” Our patients need to know that it is very important to abide by doctors’ orders for medications. If there are any drug interactions, we need to be aware of what they might be so that we can communicate that with the physician.
Primary/Secondary and Desirable/Undesirable Effects
There is a reason why we take medications; it is because we want the primary, desirable effect. But for every medication that is available, there will be secondary impacts. Sometimes those secondary effects are desirable, as may be the case when we use medications off-label. Then there are the undesirable effects - the bad side effects that can occur with medications (Figure 3).
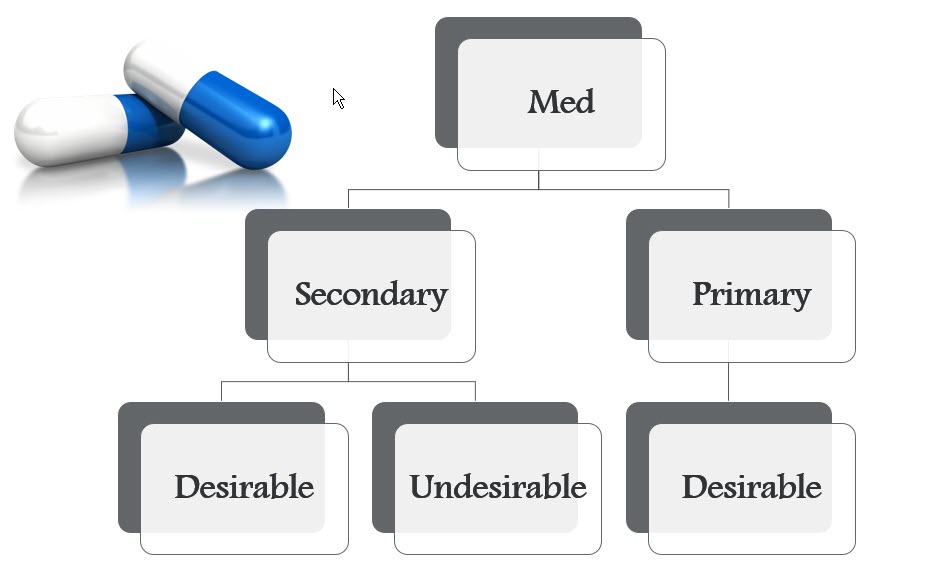
Figure 3. Medication effects.
Many times, the medications we are consuming are metabolized via first pass metabolism. This is when the medication goes through the gastrointestinal (GI) system to the liver, where it is metabolized, and then it is sent through the circulatory system to the various body parts where it needs to have its desired effect. When the liver is not functioning properly - and again, with aging it decreases in size - or the blood flow is not what it should be, the medication may not work very well. Drugs that have first pass metabolism lose some of their bioavailability; that is, the amount of drug that you have available in your bloodstream after it is metabolized. We lose some of the medication during that process. That is why you often have a higher dose because we need to take that into consideration.
